 Now in the world, perhaps, there is no adult who would not know what HIV infection is. The "plague of the 20th century" has confidently stepped into the 21st century and continues to progress. The prevalence of HIV is now the nature of a real pandemic. HIV infection has captured almost all countries. In 2004, there were about 40 million people living with HIV in the world - about 38 million adults and 2 million children. AT Russian Federation the prevalence of HIV-infected people in 2003 was 187 people per 100,000 population.
Now in the world, perhaps, there is no adult who would not know what HIV infection is. The "plague of the 20th century" has confidently stepped into the 21st century and continues to progress. The prevalence of HIV is now the nature of a real pandemic. HIV infection has captured almost all countries. In 2004, there were about 40 million people living with HIV in the world - about 38 million adults and 2 million children. AT Russian Federation the prevalence of HIV-infected people in 2003 was 187 people per 100,000 population.
According to statistics, about 8500 people are infected every day in the world, and in Russia at least 100.
Basic concepts:
HIV The human immunodeficiency virus is the causative agent of HIV infection.
is an infectious disease caused by HIV and resulting in AIDS.
AIDS Acquired Immune Deficiency Syndrome is the final stage of HIV infection, when a person's immune system is so affected that it becomes unable to resist any type of infection. Any infection, even the most harmless, can lead to serious illness and death.

History of HIV infection
In the summer of 1981, the US Centers for Disease Control published a report describing 5 cases of pneumocystis pneumonia and 26 cases of Kaposi's sarcoma in previously healthy homosexual men from Los Angeles and New York.
Over the next few months, cases were reported among injecting drug users, and shortly thereafter in people who had undergone blood transfusions.
In 1982, the diagnosis of AIDS was formulated, but the causes of its occurrence were not established.
In 1983, it was first identified HIV from cell culture of a sick person.
In 1984 it was found that HIV is the reason AIDS.
In 1985, a diagnostic method was developed HIV infections using enzyme-linked immunosorbent assay (ELISA), which detects antibodies to HIV in blood.
In 1987 the first case HIV infections registered in Russia - it was a homosexual man who worked as an interpreter in African countries.
Where did HIV come from?
In search of an answer to this question, many different theories have been proposed. Nobody can answer it exactly.
However, it is known that in the first study of the epidemiology of HIV infection, it was found that the maximum prevalence of HIV occurs in the area Central Africa. In addition, a virus capable of causing AIDS in humans has been isolated from the blood of great apes (chimpanzees) living in this area, which may indicate the possibility of infection from these monkeys - possibly by biting or butchering carcasses.
There is an assumption that HIV existed long time among the tribal settlements of Central Africa, and only in the twentieth century as a result of increased population migration spread throughout the world.
AIDS virus
HIV (human immunodeficiency virus) belongs to a subfamily of retroviruses called lentiviruses (or "slow" viruses). This means that from the moment of infection to the appearance of the first signs of the disease, and even more so before the development of AIDS, a long period of time passes, sometimes several years. Half of those infected with HIV have an asymptomatic period of about 10 years.
There are 2 types of HIV - HIV-1 and HIV-2. HIV-1 is the most common in the world, HIV-2 is closer in morphology to the simian immunodeficiency virus - the same one that was found in the blood of chimpanzees.
* - In 2019, a team of scientists in the US discovered a new strain of HIV for the first time in almost 20 years. This strain is part of the M group of the HIV-1 species. HIV has many different subtypes or strains. Like other viruses, it can change and mutate over time. This is the first new strain of the M group discovered since the principles of subtype classification were established in 2000.
When it enters the bloodstream, HIV selectively attaches to the blood cells responsible for immunity, which is due to the presence on the surface of these cells of specific CD 4 molecules that HIV recognizes. Inside these cells, HIV actively multiplies and even before the formation of any immune response, it quickly spreads throughout the body. First of all, it affects the lymph nodes, since they contain a large number of immune cells.
Throughout the illness, an effective immune response to HIV is never formed. First of all, this is due to the defeat of immune cells and the insufficiency of their function. In addition, HIV has a pronounced variability, which leads to the fact that immune cells simply cannot “recognize” the virus.
With the progression of the disease, HIV leads to the defeat of an increasing number of immune cells - CD 4 lymphocytes, the number of which gradually decreases, eventually reaching a critical number, which can be considered the beginning of AIDS.
How can you get HIV infection
- During sexual contact.
Sexual contact is the most common way of HIV transmission worldwide. Sperm contains a large amount of the virus; apparently, HIV tends to accumulate in semen, especially in inflammatory diseases - urethritis, epididymitis, when semen contains a large number of inflammatory cells containing HIV. Therefore, the risk of HIV transmission increases with concomitant sexually transmitted infections. In addition, concomitant genital infections are often accompanied by the appearance of various formations that violate the integrity of the genital mucosa - ulcers, cracks, vesicles, etc.
HIV is also found in the discharge of the vagina and cervix.
It should also be remembered criminal liability(Article 122 of the Criminal Code of the Russian Federation), which is carried by an HIV-positive partner, putting the other in a situation that is dangerous in terms of contracting HIV infection. In the same art. 122, a note was added, on the basis of which a person is released from criminal liability if the partner was warned in a timely manner about the presence of HIV infection and voluntarily agreed to take actions that created the risk of infection.
During anal intercourse, the risk of transmission of the virus from semen through the thin mucous membrane of the rectum is extremely high. In addition, during anal sex, the risk of injury to the rectal mucosa increases, which means that direct contact with blood is formed.
In heterosexual intercourse, the risk of infection from a man to a woman is about 20 times higher than from a woman to a man. This is due to the fact that the duration of contact of the vaginal mucosa with infected sperm is much longer than the duration of contact of the penis with the vaginal mucosa.
During oral sex, the risk of infection is much lower than during anal sex. However, it has been reliably proven that this risk exists! Condom use reduces but does NOT eliminate HIV infection.
- When using only syringes or needles among injecting drug users.
- When transfusing blood and its components.
It is impossible to become infected with the introduction of normal immunoglobulin and specific immunoglobulins, since these drugs are specially processed to completely inactivate the virus. After the introduction of mandatory testing of donors for HIV , the risk of infection is significantly reduced; however, the presence of a “blind period”, when the donor is already infected, but antibodies have not yet been formed, does not completely protect recipients from infection.
- From mother to child.
Infection of the fetus can occur during pregnancy - the virus is able to cross the placenta; as well as during childbirth. The risk of infecting a child from an HIV-infected mother is 12.9% in European countries and reaches 45-48% in African countries. The risk depends on the quality of medical care and treatment of the mother during pregnancy, the health of the mother, and the stage of HIV infection.
In addition, there is a clear risk of infection through breastfeeding. The virus was found in colostrum and breast milk HIV-infected women. That's why is a contraindication for breastfeeding.
- From patients to medical staff and vice versa.
The risk of infection when injured with sharp objects contaminated with the blood of HIV-infected people is about 0.3%. The risk of contact with mucous membranes and damaged skin of infected blood is even lower.
The risk of HIV transmission from an infected healthcare worker to a patient is theoretically difficult to imagine. However, in 1990, a report was published in the United States about the infection of 5 patients from an HIV-infected dentist, but the mechanism of infection remained a mystery. Subsequent observations of patients who were treated by HIV-infected surgeons, gynecologists, obstetricians, dentists did not reveal a single fact of infection.
How not to get HIV
If there is an HIV-infected person in your environment, you must remember that you cannot get infected HIV at:
- Coughing and sneezing.
- Handshake.
- Hugs and kisses.
- Eating shared food or drinks.
- In pools, baths, saunas.
- Through "injections" in transport and the subway. Information about the possible infection through infected needles that HIV-infected people put on the seats, or try to prick people in the crowd with them, is nothing more than myths. The virus persists in the environment for a very short time, in addition, the content of the virus at the tip of the needle is too small.
Saliva and other bodily fluids contain too little virus to cause infection. There is a risk of infection if body fluids (saliva, sweat, tears, urine, feces) contain blood.
HIV symptoms
Acute febrile phase
The acute febrile phase appears approximately 3-6 weeks after infection. It does not occur in all patients - approximately 50-70%. In the rest, after the incubation period, the asymptomatic phase immediately begins.
Manifestations of the acute febrile phase are nonspecific:
- Fever: fever, more often subfebrile condition, i.e. not higher than 37.5ºС.
- Sore throat.
- Enlarged lymph nodes: the appearance of painful swelling on the neck, armpits, groin.
- Headache, eye pain.
- Pain in muscles and joints.
- Drowsiness, malaise, loss of appetite, weight loss.
- Nausea, vomiting, diarrhea.
- Skin changes: rash on the skin, ulcers on the skin and mucous membranes.
- Serous meningitis can also develop - damage to the membranes of the brain, which is manifested by headache, photophobia.
The acute phase lasts from one to several weeks. In most patients, this is followed by an asymptomatic phase. However, approximately 10% of patients have a fulminant course of HIV infection with a sharp deterioration in the condition.
Asymptomatic phase of HIV infection
The duration of the asymptomatic phase varies widely - in half of HIV-infected people it is 10 years. The duration depends on the rate of reproduction of the virus.
During the asymptomatic phase, the number of CD 4 lymphocytes progressively decreases, a drop in their level below 200/µl indicates the presence of AIDS.
The asymptomatic phase may not have any clinical manifestations.
Some patients have lymphadenopathy - i.e. enlargement of all groups of lymph nodes.
Advanced stage of HIV - AIDS
At this stage, the so-called opportunistic infections- these are infections caused by opportunistic microorganisms that are normal inhabitants of our body and, under normal conditions, are not capable of causing disease.
There are 2 stages of AIDS:
A. Decrease in body weight by 10% compared with the original.
Fungal, viral, bacterial lesions of the skin and mucous membranes:
- Candidiasis stomatitis: thrush - white cheesy plaque on the oral mucosa.
- Hairy leukoplakia of the mouth - white plaques covered with grooves on the lateral surfaces of the tongue.
- Shingles is a manifestation of the reactivation of the varicella zoster virus, the causative agent of chickenpox. It is manifested by sharp soreness and rashes in the form of bubbles on large areas of the skin, mainly the trunk.
- Repeated frequent phenomena of herpetic infection.
In addition, patients constantly endure pharyngitis (sore throat), sinusitis (sinusitis, phronitis), otitis media (inflammation of the middle ear).
Bleeding gums, hemorrhagic rash (hemorrhage) on the skin of the hands and feet. This is due to developing thrombocytopenia, i.e. a decrease in the number of platelets - blood cells involved in clotting.
B. Decrease in body weight by more than 10% of the original.
At the same time, others join the above infections:
- Unexplained diarrhea and/or fever for more than 1 month.
- Tuberculosis of the lungs and other organs.
- Toxoplasmosis.
- Helminthiasis of the intestine.
- Pneumocystis pneumonia.
- Kaposi's sarcoma.
- Lymphomas.
In addition, there are severe neurological disorders.
When to suspect HIV infection
- Fever of unknown origin for more than 1 week.
- An increase in various groups of lymph nodes: cervical, axillary, inguinal - without apparent reason(absence of inflammatory diseases), especially if the lymphadenopathy does not go away within a few weeks.
- Diarrhea for several weeks.
- The appearance of signs of candidiasis (thrush) of the oral cavity in an adult.
- Extensive or atypical localization of herpetic eruptions.
- Sudden weight loss for any reason.
Who is at higher risk of contracting HIV
- injection drug addicts.
- Homosexuals.
- Prostitutes.
- Persons who practice anal sex.
- Persons with multiple sexual partners, especially if they do not use condoms.
- Persons suffering from other sexually transmitted diseases.
- Persons in need of transfusions of blood and its components.
- Persons in need of hemodialysis ("artificial kidney").
- Children whose mothers are infected.
- Health care workers, especially those in contact with HIV-infected patients.
Prevention of HIV infection
Unfortunately, no effective vaccine against HIV has been developed to date, although many countries are now conducting thorough research in this area, on which great hopes are placed.
However, so far, the prevention of HIV infection is reduced only to general preventive measures:
- Safe sex and a constant, reliable sexual partner.
Using condoms helps reduce the risk of infection, but even when used correctly, a condom is never 100% protective.
Rules for using a condom:
- the condom must be the right size.
- It is necessary to use a condom from the very beginning of sexual intercourse until completion.
- the use of condoms with nonoxynol-9 (spermicide) does not reduce the risk of infection, since it often leads to irritation of the mucous membrane, and, consequently, to microtrauma and cracks, which only contributes to infection.
- air must not remain in the receptacle - this may contribute to the rupture of the condom.
If sexual partners want to be sure that there is no risk of infection, they should both be tested for HIV.
- Refusal to use drugs. If coping with addiction is not possible, use only disposable needles and never share needles or syringes
- HIV-infected mothers should avoid breastfeeding.
Medical prophylaxis has been developed for suspected HIV infection. It consists in taking antiretroviral drugs, as in the treatment of patients with HIV, only in different dosages. The course of preventive treatment will be prescribed by the doctor of the AIDS center at an internal appointment.
HIV test
Early diagnosis of HIV is essential for successful treatment and prolongation of life in these patients.
When should I get tested for HIV?
- after sexual contact (vaginal, anal or oral) with a new partner without a condom (or if the condom broke). after sexual abuse.
- if your sexual partner has had sex with someone else.
- if your current or past sexual partner is HIV positive.
- after using the same needles or syringes for injecting drugs or other substances, or for tattoos and piercings.
- after any contact with the blood of an HIV-infected person.
- if your partner used someone else's needles or was exposed to any other risk of infection.
- after detection of any other sexually transmitted infection.
Most often, the diagnosis of HIV infection is carried out by methods that determine antibodies to HIV in the blood - i.e. specific proteins that are formed in the body of an infected person in response to a virus. The formation of antibodies occurs within 3 weeks to 6 months after infection. Therefore, an HIV test becomes possible only after this period of time, the final analysis is recommended to be performed 6 months after the alleged infection. Standard method for the determination of antibodies to HIV called enzyme immunoassay (ELISA) or ELISA. This method is very reliable, with a sensitivity of over 99.5%. Test results may be positive, negative, or questionable.
If the result is negative and there is no suspicion of recent (within the last 6 months) infection, the HIV diagnosis can be considered unconfirmed. If there is a suspicion of a recent infection, a re-examination is carried out.
There is a problem of so-called false positive results, therefore, when a positive or doubtful answer is received, the result is always checked by a more specific method. This method is called immunoblotting. The result can also be positive, negative or questionable. Upon receipt of a positive result, the diagnosis of HIV infection is considered confirmed. If the answer is doubtful, a second study is required after 4-6 weeks. If the result of the repeated immunoblot remains doubtful, the diagnosis of HIV infection is unlikely. However, for its final exclusion, immunoblotting is repeated 2 more times with an interval of 3 months or other diagnostic methods are used.
In addition to serological methods (i.e. detection of antibodies), there are methods for direct detection of HIV, which can be used to determine the DNA and RNA of the virus. These methods are based on PCR (polymerase chain reaction) and are very accurate methods for diagnosing infectious diseases. PCR can be used for early diagnosis of HIV - 2-3 weeks after doubtful exposure. However, due to the high cost and high number of false-positive results due to contamination of the test samples, these methods are used in cases where standard methods do not allow for the diagnosis or exclusion of HIV with certainty.
Video about what HIV tests you need to take and why:
Drug treatment of HIV infection and AIDS
Treatment consists in the appointment of antiviral - antiretroviral therapy; and in the treatment and prevention of opportunistic infections.
After establishing the diagnosis and registering, a series of studies are carried out to determine the stage and activity of the disease. An important indicator of the stage of the process is the level of CD 4 lymphocytes - the very cells that affect HIV, and the number of which is progressively decreasing. When the number of CD 4 lymphocytes is less than 200/µl, the risk of opportunistic infection, and, therefore, AIDS becomes significant. In addition, to determine the progression of the disease, the concentration of viral RNA in the blood is determined. Diagnostic studies should be carried out regularly, because the course HIV infections It is difficult to predict, and early diagnosis and treatment of concomitant infections is the basis for prolonging life and improving its quality.
Antiretrovirals:
The appointment of antiretroviral agents and the choice of a particular drug is the decision of a specialist doctor, which he takes depending on the patient's condition.
- Zidovudine (Retrovir) is the first antiretroviral drug. Currently, zidovudine is prescribed in combination with other drugs when the CD 4 lymphocyte count is below 500/µl. Zidovudine monotherapy is prescribed only for pregnant women to reduce the risk of fetal infection.
Side effects: impaired hematopoietic function, headache, nausea, myopathy, liver enlargement
- Didanosine (Videx) - used at the first stage of treatment HIV and after prolonged treatment with zidovudine. More often, didanosine is used in combination with other drugs.
Side effects: pancreatitis, peripheral neuritis with severe pain, nausea, diarrhea.
- Zalcitabine (Khivid) - is prescribed for the ineffectiveness or intolerance of zidovudine, as well as in combination with zidovudine at the initial stage of treatment.
Side effects: peripheral neuritis, stomatitis.
- Stavudin - used in adults in advanced stages HIV infections.
Side effects: peripheral neuritis.
- Nevirapine and delavirdine: given in combination with other antiretrovirals in adults with signs of progression HIV infections.
Side effects: maculopapular rash, which usually resolves on its own and does not require discontinuation of the drug.
- Saquinavir is a drug belonging to the group of protease inhibitors. HIV. The first drug from this group, approved for use. Saquinavir is used in advanced stages HIV infections in combination with the above antiretroviral agents.
Side effects: headache, nausea and diarrhea, increased liver enzymes, increased blood sugar levels.
- Ritonavir is approved for use both as monotherapy and in combination with other antiretroviral drugs.
Side effects: nausea, diarrhea, abdominal pain, lip paresthesia.
- Indinavir - used to treat HIV infections in adult patients.
Side effects: urolithiasis disease, increased blood bilirubin.
- Nelfinavir is approved for use in both adults and children.
The main side effect is diarrhea, which occurs in 20% of patients.
Antiretrovirals should be provided to patients registered with the AIDS Center free of charge. In addition to antiretroviral drugs, treatment HIV infections consists in an adequate selection of antimicrobial, antiviral, antifungal, and antitumor agents for the treatment of manifestations and complications AIDS.
Prevention of opportunistic infections
Prevention of opportunistic infections helps to increase the duration and improve the quality of life of patients AIDS m.
- Prevention of tuberculosis: for the timely detection of persons infected with mycobacterium tuberculosis, all HIV-infected persons undergo an annual Mantoux test. In case of a negative reaction (i.e., in the absence of an immune response to tuberculin), it is recommended to take anti-tuberculosis drugs for a year.
- Prevention of pneumocystis pneumonia is carried out in all HIV-infected patients with a decrease in CD 4 lymphocytes below 200 / μl, as well as with a fever of unknown origin with a temperature above 37.8 ° C that persists for more than 2 weeks. Prevention is carried out with biseptol.
Opportunistic infections- these are infections caused by opportunistic microorganisms that are normal inhabitants of our body, and under normal conditions are not capable of causing disease.
- Toxoplasmosis is caused by Toxoplasma gondii. The disease is manifested by toxoplasmic encephalitis, i.e. damage to the substance of the brain, with the development of epileptic seizures, hemiparesis (paralysis of half of the body), aphasia (lack of speech). In addition, confusion, stupor, coma are possible.
- Intestinal helminthiasis - pathogens are many helminths (worms). In patients AIDS can lead to severe diarrhea and dehydration.
- Tuberculosis . Mycobacterium tuberculosis is common even among healthy individuals, but they can cause disease only if the immune system is impaired. That is why the majority of HIV-infected people are prone to developing active tuberculosis, including its severe forms. Approximately 60-80% of HIV-infected tuberculosis occurs with damage to the lungs, in 30-40% - with damage to other organs.
- Bacterial pneumonia . The most common pathogens are Staphylococcus aureus and pneumococcus. Often pneumonia is severe with the development of generalized forms of infection, i.e. ingestion and reproduction of bacteria in the blood - sepsis.
- Intestinal infections – salmonellosis, dysentery, typhoid fever. Even mild forms of the disease, which in healthy people pass without treatment, in HIV-infected people proceed for a long time with numerous complications, prolonged diarrhea and generalization of the infection.
- Syphilis – in HIV-infected people, such complex and rare forms of syphilis as neurosyphilis, syphilitic nephritis (kidney damage) are more common. Complications of syphilis develop faster in AIDS patients, sometimes even with intensive treatment.
- Pneumocystis pneumonia . The causative agent of pneumocystis pneumonia is a normal inhabitant of the lungs, however, with a decrease in immunity, it can cause severe pneumonia. The causative agent is usually attributed to fungi. Pneumocystis pneumonia develops at least once in 50% of HIV-infected people. Typical symptoms of Pneumocystis pneumonia are: fever, cough with a small amount of sputum, pain in chest, aggravated by inhalation. Subsequently, shortness of breath may occur with physical activity, weight loss.
- Candidiasis is the most common fungal infection in HIV-infected people, since the causative agent, Candida albicans, is normally found in large numbers on the mucous membranes of the mouth, nose, and urinary tract. In one form or another, candidiasis occurs in all HIV-infected patients. Candidiasis (or thrush) manifests itself as a white cheesy coating on the palate, tongue, cheeks, pharynx, in vaginal discharge. In the later stages of AIDS, candidiasis of the esophagus, trachea, bronchi and lungs is possible.
- Cryptococcosis is the leading cause of meningitis (inflammation of the lining of the brain) among HIV-infected patients. The causative agent - a yeast fungus - enters the body through the respiratory tract, but in most cases it affects the brain and its membranes. The manifestations of cryptococcosis are: fever, nausea and vomiting, impaired consciousness, headache. There are also pulmonary forms of cryptococcal infection - which are accompanied by cough, shortness of breath, hemoptysis. In more than half of patients, the fungus penetrates and multiplies in the blood.
- herpetic infection. HIV-infected people are characterized by frequent recurrences of herpes of the face, oral cavity, genital organs and perianal region. As the disease progresses, the frequency and intensity of relapses increases. Herpetic lesions do not heal for a long time, leading to extremely painful and extensive damage to the skin and mucous membranes.
- Hepatitis – more than 95% of HIV-infected people are infected with hepatitis B virus, many of them also have co-infection with hepatitis D virus. Active hepatitis B is rare in HIV-infected people, but hepatitis D in these patients is severe.
Neoplasms in HIV infection
In addition to an increased susceptibility to infections, patients AIDS the tendency to form both benign and malignant tumors increases, since the control of neoplasms is also carried out by the immune system, in particular CD4 lymphocytes.
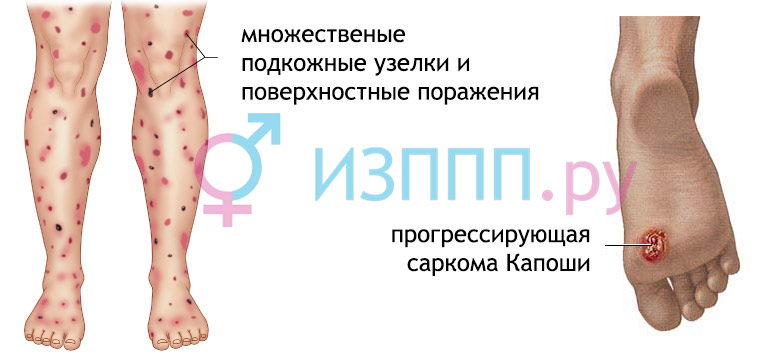
- Kaposi's sarcoma is a vascular tumor that can affect the skin, mucous membranes and internal organs. The clinical manifestations of Kaposi's sarcoma are varied. Initial manifestations appear as small red-purple nodules rising above the surface of the skin, which occur most often in exposed areas most exposed to direct sunlight. With progression, the nodes can merge, disfiguring the skin and, if located on the legs, limiting physical activity. Of the internal organs, Kaposi's sarcoma most often affects gastrointestinal tract and lungs, but sometimes the brain and heart.
- Lymphomas are late manifestations HIV infections. Lymphomas can affect both the lymph nodes and internal organs, including the brain and spinal cord. Clinical manifestations depend on the location of the lymphoma, but are almost always accompanied by fever, weight loss, and night sweats. Lymphomas can be manifested by rapidly growing volumetric formations in the oral cavity, epileptic seizures, headache, etc.
- Other malignancies - in HIV-infected people occur with the same frequency as in the general population. However, in patients HIV they have a rapid course and are difficult to treat.
Neurological disorders
- AIDS-dement syndrome;
dementia- this is a progressive decline in intelligence, which is manifested by a violation of attention and the ability to concentrate, memory impairment, difficulty in reading and solving problems.
In addition, manifestations of AIDS-dementia syndrome are motor and behavioral disorders: impaired ability to maintain a certain posture, difficulty walking, tremor (twitching of various parts of the body), apathy.
In the later stages of AIDS dementia syndrome, urinary and fecal incontinence may join, in some cases a vegetative state develops.
Severe AIDS-dementia syndrome develops in 25% of HIV-infected people.
The cause of the syndrome has not been definitively established. It is believed that it is due to the direct effect of the virus on the brain and spinal cord.
- epileptic seizures;
The causes of epileptic seizures can be both opportunistic infections that affect the brain, and neoplasms or AIDS dementia syndrome.
The most common causes are: toxoplasma encephalitis, cerebral lymphoma, cryptococcal meningitis and AIDS dementia syndrome.
- neuropathy;
A common complication of HIV infection that can occur at any stage. Clinical manifestations are varied. On the early stages it can occur in the form of progressive muscle weakness, a slight violation of sensitivity. In the future, manifestations can progress, burning pains in the legs join.
Living with HIV
Positive HIV test… What to do about it? How to react? How to live on?
First, try to overcome the panic as quickly as possible. Yes, AIDS fatal disease, but before development AIDS You can live 10 or even 20 years. In addition, now scientists around the world are actively engaged in the search for effective drugs, many recently developed drugs really significantly prolong life and improve the well-being of patients AIDS. No one knows what science will reach in this area in 5-10 years.
FROM HIV you need to learn how to live. Unfortunately, life will never be the same again. For a long time (perhaps many years) no signs of illness may occur, a person feels completely healthy and full of strength. But do not forget about infection.
First of all, you need to protect your loved ones - they must know about the infection. It can be very difficult to tell parents, a loved one about HIV-positive analysis. But no matter how difficult it is, loved ones should not be at risk, so the partner (s) (both current and former) must be informed of the result of the analysis.
Any sex, even with a condom, can be dangerous in terms of transmission of the virus, even if sometimes the danger is extremely small. Therefore, when a new partner appears, you need to give a person the opportunity to make his own choice. It must be remembered that not only vaginal or anal sex can be dangerous, but also oral.
Medical supervision:
Despite the fact that there may be no signs of the disease, regular monitoring of the condition is required. Usually this control is carried out in specialized AIDS-centers. Timely detection of disease progression and the onset of development AIDS, and, therefore, timely treatment is the basis for successful treatment in the future and slowing down the progression of the disease. Usually, the level of CD 4 lymphocytes is monitored, as well as the level of virus replication. In addition, the general condition of the patient is assessed, the possible presence of opportunistic infections. Normal indicators of the state of immunity allow to exclude the presence of AIDS, and, therefore, allow you to lead a normal life and not be afraid of any cold.
Pregnancy:
Most people get infected HIV In young age. Many women want to have children. They feel absolutely healthy and able to give birth and raise a child. No one can forbid the birth of a child - this is a personal matter for the mother. However, before planning a pregnancy, you need to weigh the pros and cons. After all, HIV is most likely transmitted through the placenta, as well as during childbirth through the birth canal. Is it worth exposing a child to a congenital HIV carrier, growing under constant medical supervision, taking toxic drugs? Even if the child does not get infected, he runs the risk of being left without parents before reaching the age of majority ... If, nevertheless, the decision is made, you need to take the planning of pregnancy and bearing with all responsibility and, even before pregnancy, contact the doctor of the AIDS center, who will direct your actions and review treatment.
Life with AIDS:
When the level of CD 4 lymphocytes falls below 200/μL, an opportunistic infection appears or any other signs of a reduced immune response are diagnosed. AIDS. Such people should follow a number of rules.
- Proper nutrition: you should not follow any diet, any malnutrition can be harmful. Nutrition should be high-calorie and balanced.
- Give up bad habits: alcohol and smoking
- Moderate physical exercises able to positively influence the immune status of HIV-infected
- You should discuss with your doctor the possibility of getting vaccinated against certain infections. Not all vaccines can be used in HIV-infected people. In particular, live vaccines should not be used. However, killed vaccines, as well as vaccines that are particles of microorganisms, are suitable for many people with HIV, depending on their immune status.
- It is always necessary to pay attention to the quality of food and water consumed. Fruits and vegetables must be thoroughly washed with boiled water, food must be thermally processed. Untested water must be disinfected, in some countries with a hot climate, even tap water is contaminated.
- Communication with animals: it is better to exclude any contact with unfamiliar (especially homeless) animals. At the very least, be sure to wash your hands after contact with an animal, even your own. You need to watch your pet especially carefully: try not to allow him to communicate with other animals and not to allow him to touch the garbage on the street. After a walk, be sure to wash, and it is better to wear gloves. It is also better to clean up after the animals with gloves.
- Try to limit your contact with sick, cold people. If you need to communicate, you should use a mask, wash your hands after contact with sick people.
Good day, dear readers!
In today's article, we will consider with you such a serious disease as HIV infection, and everything connected with it - the causes, how it is transmitted, the first signs, symptoms, stages of development, types, tests, tests, diagnostics, treatment, drugs, prevention and other useful information. So…
What does HIV mean?
HIV infection in children
HIV infection in children in many cases is accompanied by a delay in development (physical and psychomotor), frequent infectious diseases, pneumonitis, encephalopathy, hyperplasia of pulmonary lymph nodes, hemorrhagic syndrome. Moreover, HIV infection in children, which they acquired from infected mothers, is characterized by a faster course and progression.
 The main cause of HIV infection is infection with the human immunodeficiency virus. The cause of AIDS is also the same virus, because. AIDS is the last stage in the development of HIV infection.
The main cause of HIV infection is infection with the human immunodeficiency virus. The cause of AIDS is also the same virus, because. AIDS is the last stage in the development of HIV infection.
- a slowly developing virus belonging to the family of retroviruses (Retroviridae) and to the genus Lentivirus (Lentivirus). It is the word "lente" in Latin that means "slow", which partially characterizes this infection, which develops rather slowly from the moment it enters the body to the last stage.
The size of the human immunodeficiency virus is only about 100-120 nanometers, which is almost 60 times smaller than the diameter of a blood particle - an erythrocyte.
The complexity of HIV lies in its frequent genetic changes in the process of self-replication - almost every virus differs from its predecessor by at least 1 nucleotide.
In nature, as of 2017, 4 types of the virus are known - HIV-1 (HIV-1), HIV-2 (HIV-2), HIV-3 (HIV-3) and HIV-4 (HIV-4), each of which differs in the structure of the genome and other properties.
It is HIV-1 infection that plays the role in the basis of the disease of the majority of HIV-infected people, therefore, when the subtype number is not indicated, it is 1 that is assumed by default.
The source of HIV is people infected with the virus.
The main routes of infection are: injections (especially injection drugs), transfusions (of blood, plasma, red blood cells) or organ transplantation, unprotected sexual contact with a stranger, unnatural sex (anal, oral), trauma during childbirth, feeding the baby with breast milk (if the mother is infected), trauma during childbirth, use of non-disinfected medical or cosmetic items (scalpel, needles, scissors, tattoo machines, dental and other instruments).
For HIV infection and its further spread throughout the body and development, it is necessary that the infected blood, mucus, sperm and other biomaterials of the patient enter the bloodstream or lymphatic system of a person.
An interesting fact is that some people in the body have an innate defense against the human immunodeficiency virus, so they are resistant to HIV. The following elements have such protective properties: the CCR5 protein, the TRIM5a protein, the CAML protein (calcium-modulated cyclophilin ligand), and the interferon-induced transmembrane protein CD317/BST-2 (“tetherin”).
By the way, the CD317 protein, in addition to retroviruses, also actively counteracts arenaviruses, filoviruses and herpesviruses. The cofactor for CD317 is the cellular protein BCA2.
HIV Risk Groups
- Drug addicts, predominantly injecting drug users;
- Sexual partners of drug addicts;
- Persons leading a promiscuous sex life, as well as those who engage in unnatural sex;
- Prostitutes and their clients;
- Donors and people in need of a blood transfusion or organ transplant;
- Sick people with sexually transmitted diseases;
- Doctors.
The classification of HIV infection is as follows:
Classification according to clinical manifestations (in the Russian Federation and some CIS countries):
 1. Stage of incubation.
1. Stage of incubation.
2. The stage of primary manifestations, which, according to the course options, can be:
- without clinical manifestations (asymptomatic);
- acute course without secondary diseases;
- acute course with secondary diseases;
3. Subclinical stage.
4. The stage of secondary diseases caused by damage to the body by viruses, bacteria, fungi and other types of infection that develop against a background of weakened immunity. Downstream it is subdivided into:
A) body weight decreases by less than 10%, as well as frequently recurring, infectious diseases skin and mucous membranes - pharyngitis, otitis media, herpes zoster, angular cheilitis ();
B) body weight decreases by more than 10%, as well as persistent and often recurring infectious diseases of the skin, mucous membranes and internal organs - sinusitis, pharyngitis, shingles, or diarrhea (diarrhea) for a month, localized Kaposi's sarcoma;
C) body weight is significantly reduced (cachexia), as well as persistent generalized infectious diseases of the respiratory, digestive, nervous and other systems - candidiasis (trachea, bronchi, lungs, esophagus), pneumocystis pneumonia, extrapulmonary tuberculosis, herpes, encephalopathy, meningitis, cancerous tumors (disseminated Kaposi's sarcoma).
All variants of the course of the 4th stage have the following phases:
- progression of pathology in the absence of highly active antiretroviral therapy (HAART);
- progression of pathology on the background of HAART;
- remission during or after HAART.
5. Terminal stage (AIDS).
The above classification largely coincides with the classification approved by the World Health Organization (WHO).
Classification by clinical manifestations (CDC - US Centers for Disease Control and Prevention):
The CDC classification includes not only the clinical manifestations of the disease, but also the number of CD4 + -T-lymphocytes in 1 μl of blood. It is based on the division of HIV infection into just 2 categories: the disease itself and AIDS. If the parameters below meet criteria A3, B3, C1, C2 and C3, the patient is considered to have AIDS.

Symptoms according to CDC category:
A (acute retroviral syndrome) - characterized by an asymptomatic course or generalized lymphadenopathy (GLAP).
B (AIDS-associated complex syndromes) - may be accompanied by oral candidiasis, herpes zoster, cervical dysplasia, peripheral neuropathy, organic damage, idiopathic thrombocytopenia, leukoplakia, or listeriosis.
C (AIDS) - may be accompanied by candidiasis of the respiratory tract (from the oropharynx to the lungs) and / or esophagus, pneumocystosis, pneumonia, herpetic esophagitis, HIV encephalopathy, isosporosis, histoplasmosis, mycobacteriosis, cytomegalovirus infection, cryptosporidiosis, coccidioidosis, cervical cancer, Kaposi's sarcoma, lymphoma, salmonellosis and other diseases.
Diagnosis of HIV infection
Diagnosis of HIV infection includes the following examination methods:
- Anamnesis;
- Visual examination of the patient;
- Screening test (detection of blood antibodies to infection by enzyme immunoassay - ELISA);
- A test confirming the presence of antibodies in the blood (blood test by immune blotting (blot)), which is carried out only if the screening test is positive;
- Polymerase chain reaction (PCR);
- Tests for immune status (counting CD4 + lymphocytes - performed using automatic analyzers (flow cytometry method) or manually, using microscopes);
- Viral load analysis (counting the number of copies of HIV RNA in a milliliter of blood plasma);
- Rapid HIV tests - diagnostics is performed using ELISA on test strips, agglutination reaction, immunochromatography or immunological filtration analysis.
Tests alone are not enough to make a diagnosis of AIDS. Confirmation occurs only with the additional presence of 2 or more opportunistic diseases associated with this syndrome.

HIV infection - treatment
 Treatment of HIV infection is possible only after a thorough diagnosis. However, unfortunately, as of 2017, officially, adequate therapy and drugs that would completely eliminate the human immunodeficiency virus and cure the patient have not been established.
Treatment of HIV infection is possible only after a thorough diagnosis. However, unfortunately, as of 2017, officially, adequate therapy and drugs that would completely eliminate the human immunodeficiency virus and cure the patient have not been established.
the only modern method Treatment of HIV infection today is highly active antiretroviral therapy (HAART), which is aimed at slowing the progression of the disease and stopping its transition from the stage of AIDS. Thanks to HAART, a person's life can last for several decades, the only condition is the life-long intake of appropriate medications.
The insidiousness of the human immunodeficiency virus is also its mutation. So, if the drugs against HIV are not changed after a certain time, which is determined on the basis of constant monitoring of the disease, the virus adapts, and the prescribed treatment regimen becomes ineffective. Therefore, at different intervals, the doctor changes the treatment regimen, and with it the medications. The reason for changing the drug can also be its individual intolerance by the patient.
Modern drug development aims not only to achieve the goal of effectiveness against HIV, but also to reduce the side effects of them.
The effectiveness of treatment also increases with a change in a person's lifestyle, improving its quality - healthy sleep, proper nutrition, stress avoidance, active lifestyle, positive emotions, etc.
Thus, the following points in the treatment of HIV infection can be distinguished:
- Drug treatment of HIV infection;
- Diet;
- Preventive actions.
Important! Before using drugs, be sure to consult your doctor for advice!
1. Drug treatment of HIV infection
At the beginning, it is necessary to immediately remind once again that AIDS is the last stage in the development of HIV infection, and it is at this stage that a person usually has very little time left to live. Therefore, it is very important to prevent the development of AIDS, and this largely depends on the timely diagnosis and adequate treatment of HIV infection. We also noted that the only treatment for HIV today is highly active antiretroviral therapy, which, according to statistics, reduces the risk of developing AIDS to almost 1-2%.
Highly active antiretroviral therapy (HAART)- a method of treating HIV infection based on the simultaneous administration of three or four drugs (tritherapy). The number of drugs is associated with the mutagenicity of the virus, and in order to bind it at this stage for as long as possible, the doctor selects exactly the complex of drugs. Each of the drugs, depending on the principle of action, is included in a separate group - reverse transcriptase inhibitors (nucleoside and non-nucleoside), integrase inhibitors, protease inhibitors, receptor inhibitors and fusion inhibitors (fusion inhibitors).
HAART has the following goals:
- Virological - aimed at arresting the reproduction and spread of HIV, an indicator of which is a decrease in viral load by 10 or more times in just 30 days, to 20-50 copies / ml or less in 16-24 weeks, as well as keeping these indicators as long as possible;
- Immunological - aimed at restoring the normal functioning and health of the immune system, which is due to the restoration of the number of CD4-lymphocytes and an adequate immune response to infection;
- Clinical - aimed at preventing the formation of secondary infectious diseases and AIDS, it makes it possible to conceive a child.
Medicines for HIV infection
Nucleoside reverse transcriptase inhibitors- the mechanism of action is based on the competitive suppression of the HIV enzyme, which ensures the creation of DNA, which is based on the RNA of the virus. It is the first group of drugs against retroviruses. They are well tolerated. Among the side effects can be identified - lactic acidosis, bone marrow suppression, polyneuropathy and lipoatrophy. The substance is excreted from the body through the kidneys.
Among the nucleoside reverse transcriptase inhibitors are abacavir (Ziagen), zidovudine (Azidothymidine, Zidovirin, Retrovir, Timazid), lamivudine (Virolam, Heptavir-150, Lamivudine-3TS ”, “Epivir”), stavudine (“Aktastav”, “Zerit”, “Stavudin”), tenofovir (“Viread”, “Tenvir”), phosphazide (“Nikavir”), emtricitabine (“Emtriva”), as well as complexes abacavir + lamivudine (Kivexa, Epzicom), zidovudine + lamivudine (Combivir), tenofovir + emtricitabine (Truvada), and zidovudine + lamivudine + abacavir (Trizivir).
Non-nucleoside reverse transcriptase inhibitors- delavirdine (Rescriptor), nevirapine (Viramun), rilpivirine (Edurant), efavirenz (Regast, Sustiva), etravirine (Intelence).
Integrase inhibitors- the mechanism of action is based on blocking the virus enzyme, which is involved in the integration of viral DNA into the genome of the target cell, after which a provirus is formed.
Integrase inhibitors include dolutegravir (Tivicay), raltegravir (Isentress), elvitegravir (Vitekta).
Protease inhibitors- the mechanism of action is based on blocking the virus protease enzyme (retropepsin), which is directly involved in the cleavage of Gag-Pol polyproteins into individual proteins, after which the mature proteins of the human immunodeficiency virus virion are actually formed.
Protease inhibitors include amprenavir (Agenerasa), darunavir (Prezista), indinavir (Crixivan), nelfinavir (Viracept), ritonavir (Norvir, Ritonavir), saquinavir-INV ( Invirase), tipranavir (Aptivus), fosamprenavir (Lexiva, Telzir), as well as the combination drug lopinavir + ritonavir (Kaletra).
Receptor inhibitors- the mechanism of action is based on blocking the penetration of HIV into the target cell, which is due to the effect of the substance on the co-receptors CXCR4 and CCR5.
Among the receptor inhibitors, maraviroc (Celzentri) can be distinguished.
Fusion inhibitors (fusion inhibitors)- the mechanism of action is based on blocking the last stage of the introduction of the virus into the target cell.
Among the fusion inhibitors, enfuvirtide (Fuseon) can be distinguished.
The use of HAART during pregnancy reduces the risk of transmission from an infected mother to her child to 1%, although without this therapy, the infection rate of the child is about 20%.
Side effects from the use of HAART drugs include pancreatitis, anemia, skin rashes, kidney stones, peripheral neuropathy, lactic acidosis, hyperlipidemia, lipodystrophy, as well as Fanconi syndrome, Stevens-Johnson syndrome and others.
 The diet for HIV infection is aimed at preventing the patient from losing weight, as well as providing the cells of the body with the necessary energy and, of course, stimulating and maintaining the normal functioning of not only the immune system, but also other systems.
The diet for HIV infection is aimed at preventing the patient from losing weight, as well as providing the cells of the body with the necessary energy and, of course, stimulating and maintaining the normal functioning of not only the immune system, but also other systems.
It is also necessary to pay attention to a certain vulnerability of immunity weakened by infection, therefore, to protect yourself from infection with other types of infection, be sure to follow the rules of personal hygiene and the rules of cooking.
Nutrition for HIV/AIDS should:
2. Be high-calorie, which is why it is recommended to add butter, mayonnaise, cheese, sour cream to food.
3. Include plenty of drink, it is especially useful to drink decoctions and freshly squeezed juices with plenty of vitamin C, which stimulates the immune system - decoction, juices (apple, grape, cherry).
4. Be frequent, 5-6 times a day, but in small portions.
5. Water for drinking and cooking should be purified. Avoid expired foods, undercooked meats, raw eggs, and unpasteurized milk.
What can you eat with HIV infection:
- Soups - vegetable, on cereals, with vermicelli, on meat broth, it is possible with the addition of butter;
- Meat - beef, turkey, chicken, lungs, liver, lean fish (preferably sea);
- Groats - buckwheat, barley, rice, millet and oatmeal;
- Kashi - with the addition of dried fruits, honey, jam;
- Bread;
- Fats - sunflower oil, butter, margarine;
- Vegetable food (vegetables, fruits, berries) - carrots, potatoes, cabbage, zucchini, pumpkin, legumes, peas, apples, grapes, plums and others;
- Sweet - honey, jam, jam, jam, marmalade, marshmallow, sugar, sweet pastries (no more than 1 time per month).
Also, with HIV infection and AIDS, there is a shortage of such and
3. Preventive measures
Preventive measures for HIV infection that must be observed during treatment include:
- Avoiding re-exposure to infection;
- Healthy sleep;
- Compliance with the rules of personal hygiene;
- Avoiding the possibility of infection with other types of infection - and others;
- Avoidance of stress;
- Timely wet cleaning at the place of residence;
- Refusal to stay in the sun for a long time;
- Complete refusal of alcoholic products, smoking;
- Complete nutrition;
- Active lifestyle;
- Holidays at sea, in the mountains, i.e. in the most environmentally friendly places.
Additional HIV prevention measures will be discussed at the end of the article.
 Important!
Before use folk remedies against HIV infection, be sure to consult your doctor!
Important!
Before use folk remedies against HIV infection, be sure to consult your doctor!
St. John's wort. Pour well-dried chopped grass into an enameled pan and fill it with 1 liter of soft purified water, then put the container on fire. After the agent boils, boil the agent for another 1 hour over low heat, then remove, cool, strain and pour the broth into a jar. Add 50 g of sea buckthorn oil to the decoction, mix thoroughly and set aside in a cold place for infusion, for 2 days. You need to take the drug 50 g 3-4 times a day.
Licorice. Pour 50 g of crushed into an enameled pan, pour 1 liter of purified water into it and put it on the stove, over a big fire. Bringing to a boil, reduce the heat to the minimum value and simmer the remedy for about 1 hour. After removing the broth from the stove, cool it, strain, pour into a glass container, add here 3 tbsp. spoons of natural, mix. You need to drink a decoction of 1 glass in the morning, on an empty stomach.
Propolis. Pour 10 g of crushed half a glass of water and put the product in a water bath to simmer for 1 hour. Then cool the product and take it 1-3 times a day, 50 g each.
Syrup from berries, apples and nuts. Mix together in an enamel saucepan 500 g of fresh red berries, 500 g of lingonberries, 1 kg of chopped green apples, 2 cups of chopped, 2 kg of sugar and 300 ml of purified water. Set aside for a while until the sugar dissolves, then put the product on a small fire for 30 minutes and cook syrup from it. After the syrup must be cooled, poured into a jar and taken in the morning, on an empty stomach, 1 tbsp. spoon, which can be washed down with a sip of boiled water.
 HIV prevention includes:
HIV prevention includes:
- Compliance;
- Examinations of blood and organ donors;
- Examination of all pregnant women for the presence of antibodies to HIV;
- Birth control in HIV-positive women and prevention from breastfeeding;
- Conducting lessons to inform young people about the consequences of certain sexual relationships;
- There are movements to work with drug addicts, the purpose of which is psychological help, teaching about safe injections and exchange of needles and syringes;
- Decrease in the scale of drug addiction and prostitution;
- Opening rehabilitation centers for drug addicts;
- Promotion of safe sexual relations;
- Refusal of unnatural sexual relations (anal, oral sex);
- Compliance by medical workers with all safety rules for working with biomaterials of infected people, incl. diseases such as;
- If a medical worker has contact of mucous or blood (cut, puncture of the skin) with an infected biomaterial, the wound must be treated with alcohol, then washed with laundry soap and again treated with alcohol, and after that, in the first 3-4 hours, take drugs from the HAART group ( for example - "Azidothymidine"), which minimizes the possibility of developing HIV infection, and be observed by an infectious disease specialist for 1 year;
- Mandatory treatment of sexually transmitted diseases (STDs) so that they do not become chronic;
- Refusal of tattoo stuffing, as well as visits to unverified beauty salons, cosmetologists at home, little-known dental clinics with a dubious reputation;
- As of 2017, a vaccine against HIV and AIDS has not yet been officially developed, at least some drugs are still undergoing preclinical trials.
 An expression such as "People living with HIV" (PLHIV) is used to refer to a person or group of people who are HIV positive. This term was coined due to the fact that PLHIV can live in society for several decades, and die not from the infection itself, but from the natural aging of the body. PLWH should by no means be a stigma to be shunned and kept in isolation. Also, PLHIV have the same rights as an HIV-negative person - to medical care, education, work, and the birth of a child.
An expression such as "People living with HIV" (PLHIV) is used to refer to a person or group of people who are HIV positive. This term was coined due to the fact that PLHIV can live in society for several decades, and die not from the infection itself, but from the natural aging of the body. PLWH should by no means be a stigma to be shunned and kept in isolation. Also, PLHIV have the same rights as an HIV-negative person - to medical care, education, work, and the birth of a child.
Which doctor should I contact for HIV infection?
HIV infection - video
AIDS virus(abbreviation HIV) was discovered in 1983 in the study of the causes of AIDS - syndrome immunodeficiency. The first official publications about AIDS appeared back in 81, the new disease was associated with sarcoma Kaposi and unusually occurring pneumonia in homosexuals. The designation AIDS (AIDS) was fixed as a term in 82, when similar symptoms found in drug addicts, homosexuals and patients with hemophilia were combined into a single acquired immune deficiency syndrome.
Modern definition of HIV infection: a viral disease based on immunodeficiency, which causes the development of concomitant (opportunistic) infections and oncological processes.
AIDS is the last stage of HIV infection, either congenital or acquired.
How can you get HIV?
The source of infection is an HIV-infected person, and at any stage of the disease and for life. Large amounts of the virus contain blood (including menstrual) and lymph, semen, saliva, vaginal discharge, breast milk, liquor- cerebrospinal fluid, tears. endemic(with reference to the locality) the focus of HIV was detected in West Africa, monkeys were infected with the type 2 virus. The natural focus of the type 1 virus has not been found. HIV is transmitted only from person to person.
With unprotected sex the possibility of contracting HIV increases if there is inflammation, microtrauma of the skin or mucous membranes of the genitals, anus. At the only Infection is rare during sexual intercourse, but with each subsequent intercourse the probability increases. During any kind of communication receiving a sexual partner is more likely to get HIV (1 to 50 per 10,000 episodes of unprotected sex) than a transmitting partner (0.5 to 6.5). Therefore, the risk group includes prostitutes with their clients and barebackers- Gays who deliberately do not use condoms.

ways of HIV transmission
A baby can become infected with HIV in utero from an infected mother if there are defects in the placenta and the virus enters the blood of the fetus. In childbirth, infection occurs through the injured birth canal, later - through breast milk. Between 25 and 35% of children born to HIV-infected mothers may become carriers of the virus or develop AIDS.
For medical reasons: transfusions of whole blood and cell mass (platelets, erythrocytes), fresh or frozen plasma to patients. Among the medical staff, accidental injections with a contaminated needle account for 0.3-0.5% of all cases of HIV infection, so doctors are at risk.
With intravenous injections with a “public” needle or syringe, the risks of contracting HIV are more than 95%, therefore, at the moment, the majority of carriers of the virus and an inexhaustible source of infection are drug addicts constituting the main risk group for HIV.
HIV CANNOT be contracted through the household route, as well as through water in pools and baths, insect bites, air.
Spread of HIV
Features - Variable incubation period, unequal speed of occurrence and severity of symptoms, directly dependent on the state of human health. People weakened(asocials, drug addicts, residents of poor countries) or with concomitant chronic or acute STDs(, etc.), get sick more often and more severely, HIV symptoms appear faster, and life expectancy is 10-11 years from the moment of infection.
In a prosperous social environment, in practically healthy people, the incubation period can stretch for 10-20 years, the symptoms are erased and progress very slowly. With adequate treatment, such patients live a long time, and death occurs due to natural causes - due to age.
Statistics:
- At the beginning of 2014 in the world - 35 million people diagnosed with HIV;
- The increase in 2013 infected people was 2.1 million, deaths from AIDS - 1.5 million;
- The number of registered HIV carriers among the entire population of the Earth is approaching 1%;
- In the Russian Federation in 2013, there were 800 thousand infected and sick, that is, about 0.6% of the population is affected by HIV;
- 90% of all AIDS cases in Europe are in Ukraine (70%) and Russia (20%).

HIV prevalence by country (percentage of virus carriers among the adult population)
Data:
- HIV is more often detected in men than in women;
- In the last 5 years, cases of HIV detection in pregnant women have become more frequent;
- Inhabitants of the countries of the north of Europe become infected and suffer from AIDS much less frequently than the southerners;
- Africans are most susceptible to the immunodeficiency virus, approximately 2/3 of all sick and infected people are in Africa;
- Those infected with the virus over the age of 35 develop AIDS 2 times faster than young people.
Characterization of the virus
HIV belongs to the group retroviruses HTLV groups and gender lentiviruses("slow" viruses). It has the form of spherical particles, 60 times smaller than an erythrocyte in size. It dies quickly in an acidic environment, under the influence of 70% ethanol, 3% hydrogen peroxide or 0.5% formaldehyde. sensitive to heat treatment– becomes inactive after 10 minutes. Already at +560°C, at 1000°C within a minute. Resistant to UV, radiation, freezing and drying.
Blood with HIV that has fallen on various objects remains infectious for up to 1-2 weeks.
HIV is constantly changing the genome, each subsequent virus differs from the previous one by one step of the RNA chain - a nucleotide. The HIV genome is 104 nucleotides long, and the number of errors during reproduction is such that after about 5 years nothing remains of the original combinations: HIV mutates completely. Consequently, previously used drugs become ineffective, and new ones have to be invented.

Although in nature there are not even two absolutely identical HIV genomes, some groups of viruses have typical signs. On their basis, all HIV is classified into groups, numbered from 1 to 4.
- HIV-1: the most common, it was this group that was first discovered (1983).
- HIV-2: Less likely to be infected than HIV-1. Those infected with type 2 have no immunity to type 1 of the virus.
- HIV-3 and 4: rare variations, do not particularly affect the spread of HIV. In the formation of a pandemic (a general epidemic covering countries on different continents), HIV-1 and 2 are of primary importance, and HIV-2 is more common in West African countries.
Development of AIDS
Normally, the body is protected from the inside: the main role is assigned to cellular immunity, in particular lymphocytes. T-lymphocytes produces thymus (thymus gland), according to their functional duties, they are divided into T-helpers, T-killers and T-suppressors. Helpers"recognize" tumor and virus-damaged cells, and activate T-killers, which are engaged in the destruction of atypical formations. T-suppressors regulate the direction of the immune response, not allowing you to start a reaction against your own healthy tissues.

The T-lymphocyte affected by the virus becomes atypical, the immune system reacts to it as a foreign formation and “sends” T-killers to help. They destroy the former T-helper, the capsids are released and take with them a part of the lipid membrane of the lymphocyte, becoming unrecognizable to the immune system. Further, the capsids disintegrate, and new virions are introduced into other T-helpers.

Gradually, the number of helper cells decreases, and inside the human body, the “friend or foe” recognition system ceases to function. In addition to this, HIV activates the mechanism of mass apoptosis(programmed death) of all types of T-lymphocytes. The result is an active inflammatory reaction to the resident (normal, permanent) and conditionally pathogenic microflora, and at the same time, an inadequate response of the immune system to really dangerous fungi and tumor cells. Immunodeficiency syndrome develops, characteristic symptoms of AIDS appear.
Clinical manifestations
Symptoms of HIV depend on the period and stage of the disease, as well as on the form in which the effect of the virus is predominantly manifested. HIV periods divided into incubation, when there are no antibodies to the virus in the blood, and clinical - antibodies are determined, the first signs of the disease appear. AT clinical distinguish stages HIV:
- Primary, including two forms- asymptomatic and acute infection without secondary manifestations, with concomitant diseases;
- Latent;
- AIDS with secondary diseases;
- Terminal stage.
I. Incubation period, the time from the moment of HIV infection to the onset of symptoms, is called the serological window. Serum reactions to the immunodeficiency virus are negative: specific antibodies have not yet been determined. The average duration of incubation is 12 weeks; the terms can be reduced to 14 days with concomitant STDs, tuberculosis, general asthenia, or increase up to 10-20 years. During the entire period, the patient dangerous as a source of HIV infection.
II. Stage of primary manifestations of HIV characterized seroconversion- the appearance of specific antibodies, serological reactions become positive. The asymptomatic form is diagnosed only by a blood test. Acute HIV infection occurs 12 weeks after infection (50-90% of cases).
First signs manifested by fever various types rash, lymphadenitis, sore throat (pharyngitis). Possible intestinal upset - diarrhea and pain in the abdomen, enlargement of the liver and spleen. A typical laboratory finding: mononuclear lymphocytes, which are found in the blood at this stage of HIV.
Secondary diseases appear in 10-15% of cases against the background of a transient decrease in the number of T-helper lymphocytes. The severity of diseases is moderate, they are treatable. The duration of the stage is on average 2-3 weeks, in most patients it becomes latent.
Forms acute HIV infections:

III. Latent stage of HIV, lasts up to 2-20 years or more. Immunodeficiency progresses slowly, HIV symptoms are expressed lymphadenitis- Enlargement of lymph nodes. They are elastic and painless, mobile, the skin retains its normal color. When diagnosing latent HIV infection, the number of enlarged nodes is taken into account - at least two, and their localization - at least 2 groups that are not connected by a common lymph flow (the exception is the inguinal nodes). Lymph moves in the same direction as venous blood, from the periphery to the heart. If 2 lymph nodes are enlarged in the head and neck, then this is not considered a sign of the latent stage of HIV. The combined increase in groups of nodes located in the upper and lower parts of the body, plus a progressive decrease in the number of T-lymphocytes (helpers) are in favor of HIV.
IV. Secondary diseases, with periods of progression and remission, depending on the severity of manifestations, is divided into stages (4 A-B). Persistent immunodeficiency develops against the background of massive death of T-helpers and depletion of lymphocyte populations. Manifestations - various visceral (internal) and skin manifestations, Kaposi's sarcoma.
v. terminal stage irreversible changes are inherent, treatment is ineffective. The number of T-helper cells (CD4 cells) falls below 0.05x109/l, patients die weeks or months after the onset of the stage. In drug addicts who have been using psychoactive substances for several years, the level of CD4 can remain almost within the normal range, but severe infectious complications (abscesses, pneumonia, etc.) develop very quickly and lead to death.
Kaposi's sarcoma
Sarcoma ( angiosarcoma) Kaposi is a tumor that originates from the connective tissue and affects the skin, mucous membranes and internal organs. It is provoked by the herpes virus HHV-8; more common in men infected with HIV. The epidemic type is one of the reliable signs of AIDS. Kaposi's sarcoma develops in stages: begins with the appearance spots 1-5 mm in size, irregularly shaped, bright bluish-red or brown in color, with a smooth surface. With AIDS, they are bright, localized on the tip of the nose, hands, mucous membranes and on the hard palate.
Then tubercles- papules, round or semicircular, up to 10 mm in diameter, elastic to the touch, can merge into plaques with a surface similar to an orange peel. Tubercles and plaques transform into nodular tumors 1-5 cm in size, which merge with each other and are covered ulcers. At this stage, sarcoma can be confused with syphilitic gums. Syphilis is often combined with the immunodeficiency virus, like hepatitis C, shortening the incubation period and provoking fast development acute symptoms of AIDS - lymphadenitis, damage to internal organs.
Kaposi's sarcoma is clinically divided into forms- acute, subacute and chronic. Each is characterized by the rate of tumor development, complications and prognosis regarding the duration of the disease. At acute form, the process spreads rapidly, the cause of death is intoxication and extreme exhaustion ( cachexia), a lifetime of 2 months to a maximum of 2 years. At subacute the course of symptoms increases more slowly, the prognosis of life expectancy is 2-3 years; for chronic form sarcomas - 10 years, possibly more.
HIV in children
Incubation period lasts about a year if HIV has been passed from mother to fetus. When infected through the blood (parenteral) - up to 3.5 years; after transfusion of infected blood, the incubation is short, 2-4 weeks, and the symptoms are severe. HIV infection in children occurs with a primary lesion nervous system (up to 80% of cases); long-term, up to 2-3 years, bacterial inflammation; with damage to the kidneys, liver and heart.
Develops very often pneumocystis or lymphocytic pneumonia, parotid inflammation salivary glands (mumps aka a pig). HIV is congenital dysmorphic syndrome- impaired development of organs and systems, in particular microcephaly - reduced size of the head and brain. A decrease in the level of gamma globulin fraction proteins in the blood is observed in half of those infected with HIV. Highly rare Kaposi's sarcoma and hepatitis C, B.
Dysmorphic syndrome or HIV embryopathy determined in children infected with early terms of pregnancy. Manifestations: microcephaly, nose without membranes, the distance between the eyes is increased. The forehead is flat, the upper lip is split and protrudes forward. Strabismus, eyeballs protruding outward ( exophthalmos), the cornea is bluish in color. Growth retardation is observed, development does not meet the standards. Forecast for life basically negative, mortality is high during 4-9 months of life.

Manifestations of neuro-AIDS: chronic meningitis, encephalopathy(damage to brain tissue) with the development of dementia, damage to peripheral nerves with symmetrical disorders of sensitivity and trophism in the arms and legs. Children significantly lag behind their peers in development, are prone to convulsions and muscle hypertonicity, paralysis of the limbs may develop. Diagnosis of HIV neuro-symptoms is based on clinical signs, blood test data, and computed tomography findings. Layered images reveal atrophy(reduction) of the cerebral cortex, expansion of the cerebral ventricles. With HIV infection, calcium deposits are characteristic in the basal ganglions (ganglia) of the brain. The progression of encephalopathy leads to death within 12-15 months.
Pneumocystis pneumonia: in children of the 1st year of life it is observed in 75% of cases, older than a year - in 38%. Often, pneumonia develops by the age of six months, manifestations are high fever, rapid breathing, dry and persistent cough. Increased sweating, especially at night; a weakness that only gets worse with time. Pneumonia is diagnosed after auscultation (according to the stages of development, first weakened breathing is heard, then small dry rales, at the stage of resolution - crepitus, the sound is heard at the end of inspiration); x-ray (enhanced pattern, infiltration of lung fields) and microscopy of the biomaterial (pneumocysts are detected).
Lymphocytic interstitial pneumonia: a unique disease associated specifically with childhood AIDS, there are no concomitant infections. The partitions between the alveoli and the tissue around the bronchi are compacted, where lymphocytes and other immune cells are determined. Pneumonia begins imperceptibly, develops slowly, among the initial symptoms are typical prolonged dry cough and dry mucous membranes. Then shortness of breath appears and respiratory failure sharply increases. The x-ray image shows the compaction of the lung fields, enlarged lymph nodes in the mediastinum - the space between the lungs.
Lab tests for HIV
The most common method for diagnosing HIV is (ELISA or ELISA test), using it to detect the immunodeficiency virus. Antibodies to HIV are formed in the period from three weeks to 3 months after infection, they are found in 95% of cases. Six months later, HIV antibodies are found in 9% of patients, later - only in 0.5-1%.
As biomaterial using blood serum taken from a vein. You can get a false-positive ELISA result if HIV infection is accompanied by autoimmune (lupus, rheumatoid arthritis), oncological or chronic infectious diseases (tuberculosis, syphilis). A false-negative answer happens during the so-called. seronegative window, when antibodies in the blood have not yet appeared. In this case, to control the blood for HIV, you need to donate again, after a pause of 1 to 3 months.

If the ELISA is evaluated positively, the HIV test is duplicated using a polymerase chain reaction, determining the presence of virus RNA in the blood. The technique is highly sensitive and specific, does not depend on the presence of antibodies to the immunodeficiency virus. Immune blotting is also used, which makes it possible to find antibodies to HIV protein particles with an exact molecular weight (41, 120 and 160 thousand). Their identification gives the right to make a final diagnosis without confirmation by additional methods.
HIV test necessarily is done only during pregnancy, in other cases, a similar examination is a voluntary matter. Doctors do not have the right to disclose the diagnosis, all information about patients and those infected with HIV is confidential. Patients have the same rights as healthy people. Criminal punishment is provided for the deliberate spread of HIV (Article 122 of the Criminal Code of the Russian Federation).
Principles of treatment
HIV treatment is prescribed after a clinical examination and laboratory confirmation of the diagnosis. The patient is constantly under observation, repeated blood tests are carried out during antiviral therapy and after treatment of manifestations of HIV.
The cure for HIV has not yet been invented, the vaccine does not exist. It is impossible to remove the virus from the body, and this is a fact at this time. However, one should not lose hope: active antiretroviral therapy (HAART) can reliably slow down and even practically stop the development of HIV infection and its complications.
The life expectancy of patients receiving modern treatment is 38 years (for men) and 41 years (for women). An exception is the combination of HIV with hepatitis C, when less than half of patients reach the 5-year survival threshold.
HAART- a technique based on the use of several pharmaceuticals at once that affect various mechanisms for the development of HIV symptoms. Therapy combines several goals at once.
- Virological: block the reproduction of the virus in order to reduce the viral load (the number of copies of HIV in 1 ml3 of blood plasma) and fix it at a low level.
- Immunological: stabilize the immune system to raise the level of T-lymphocytes and restore the body's defense against infections.
- Clinical: to increase the period of full-fledged life of those infected with HIV, to prevent the development of AIDS and its manifestations.
Virological treatment
The human immunodeficiency virus is affected by drugs that do not allow it to attach to a T-lymphocyte and penetrate inside - this inhibitors(suppressors) penetration. A drug Celzentree.
The second group of drugs are viral protease inhibitors, which is responsible for the formation of full-fledged viruses. When it is inactivated, new viruses are formed, but they cannot infect new lymphocytes. Preparations Kaletra, Viracept, Reyataz and etc.

The third group is reverse transcriptase inhibitors, an enzyme that helps reproduce viral RNA in the nucleus of a lymphocyte. Preparations Zinovudine, Didanosine.Also use combined anti-HIV medicines that need to be taken only 1 time per day - Trizivir, Combivir, Lamivudine, Abacavir.
With simultaneous exposure to drugs, the virus cannot get inside the lymphocytes and "multiply". When appointed tritherapy the ability of HIV to mutate and develop drug insensitivity is taken into account: even if the virus becomes immune to one drug, the remaining two will work. Dosage calculated for each patient, taking into account the state of health and possible side effects. A separate scheme is used for pregnant women, and after the use of HAART, the frequency of HIV transmission from mother to child decreases from 20-35% to 1-1.2%.
It is important to take your medicines at the same time every day for the rest of your life.: if the schedule is violated or the course is interrupted, the treatment completely loses its meaning. Viruses quickly change the genome, becoming immune ( resistant) to therapy, and form numerous resistant strains. With such a development of the disease, it is very problematic to choose antiviral treatment, and sometimes it is simply impossible. Cases of resistance development are more often observed among HIV-infected drug addicts and alcoholics, for whom exact adherence to the therapy schedule is unrealistic.
The drugs are effective, but their prices are high. For example, the cost of a year's treatment with Fuzeon (a group of penetration inhibitors) reaches $25,000, and the cost per month when using Trizivir ranges from $1,000.
note that farm. funds almost always two names - according to the active substance and the commercial name of the drug, which was given to it by the manufacturer. The prescription must be written by active substance, indicating its amount in a tablet (capsule, ampoule, etc.). Substances with the same effect are often presented under different commercial names and can vary significantly in price. The job of the pharmacist is to offer the patient a choice of several options and to orient regarding the cost. Generics- analogues of original developments are always much cheaper than "branded" medicines.
Immunological and clinical treatment
 The use of an immunostimulant drug Inosine pranobex, due to which the level of lymphocytes increases, the activity of certain fractions of leukocytes is stimulated. The antiviral action indicated in the annotation does not apply to HIV. Indications relevant for HIV-infected: viral hepatitis C, B; immunodeficiency states; cytomegalovirus; virus herpes simplex type 1; mumps. Dosages: adults and children 3-4 times / day. at the rate of 50-100 mg / kg. Well 5-15 days, can be repeated many times, but only under the control of an infectious disease specialist. Contraindications: increased content uric acid in blood ( hyperuricemia), kidney stones, systemic diseases, pregnancy and breastfeeding.
The use of an immunostimulant drug Inosine pranobex, due to which the level of lymphocytes increases, the activity of certain fractions of leukocytes is stimulated. The antiviral action indicated in the annotation does not apply to HIV. Indications relevant for HIV-infected: viral hepatitis C, B; immunodeficiency states; cytomegalovirus; virus herpes simplex type 1; mumps. Dosages: adults and children 3-4 times / day. at the rate of 50-100 mg / kg. Well 5-15 days, can be repeated many times, but only under the control of an infectious disease specialist. Contraindications: increased content uric acid in blood ( hyperuricemia), kidney stones, systemic diseases, pregnancy and breastfeeding.
The drug of the interferon group Viferon has antiviral and immunomodulatory activity. In the case of HIV (or AIDS), it is used for Kaposi's sarcoma, fungal infections and hairy cell leukemia. The action of the drug is complex: interferon enhances the activity of T-helpers and increases the production of lymphocytes, blocks the reproduction of viruses in several ways. Additional components - vit.C, E - protect cells, and the effectiveness of interferon increases by 12-15 times (synergistic effect). Viferon can be taken for long courses, its activity does not decrease over time. In addition to HIV, indications are any viral infections, mycoses (including internal organs), hepatitis C, B or D. When administered rectally the drug is used twice a day for a course of 5-10 days, the ointment for HIV is not used. Pregnant women are prescribed from 14 weeks.

Treatment of pulmonary manifestations
The main early manifestation of HIV infection is inflammation of the lungs.to their caused by pneumocystis (Pneumocystis carina), single-celled organisms similar to fungi and protozoa at the same time. In patients with AIDS, untreated pneumocystis pneumonia in 40% ends in death, and correct and timely prescribed therapeutic regimens help reduce the mortality rate to 25%. With the development of relapse, the prognosis worsens, repeated pneumonia is less sensitive to treatment, and mortality reaches 60%.
Treatment: main drugs - Biseptol (Bactrim) or pentamidine. They act in different directions, but eventually lead to the death of pneumocysts. Biseptol is taken orally, pentamidine is injected into the muscles or into a vein. The course is from 14 to 30 days, with AIDS it is preferable to use pentamidine. Together, drugs are not prescribed, tk. their toxic effect is enhanced without a noticeable increase in the therapeutic effect.
Low toxicity drug DFMO (alpha-difluoromethylornithine) acts on pneumocysts and at the same time blocks the reproduction of retroviruses, which include HIV, and also has a beneficial effect on lymphocytes. The course is 2 months, the daily dosage is calculated based on 6 g per 1 sq. meter of body surface and break it into 3 doses.
With adequate treatment of pneumonia, improvement is noticeable already on the 4th-5th day from the start of therapy, a month later, in a quarter of patients, pneumocysts are not detected at all.
Immunity to HIV
Statistics of confirmed HIV resistance: among Europeans, 1% are completely immune to the immunodeficiency virus, up to 15% are partially. In both cases, the mechanisms are not clear. Scientists associate this phenomenon with epidemics of bubonic plague in Europe in the 14th and 18th centuries (Scandinavia), when, perhaps, in some people, early genetic mutations were fixed in heredity. There is also a group of so-called. "Non-progressors", which make up about 10% of those infected with HIV, in whom AIDS symptoms do not appear for a long time. In general, immunity to HIV does not exist.

A person is immune to the HIV-1 serotype if his body produces the TRIM5a protein, which is able to “recognize” the viral capsid and block HIV reproduction. The CD317 protein can keep viruses on the surface of cells, preventing them from infecting healthy lymphocytes, and CAML makes it difficult for new viruses to be released into the blood. The beneficial activity of both proteins is disrupted by hepatitis C and simple viruses, therefore, with these concomitant diseases, the risks of HIV infection are higher.
Prevention
The fight against the AIDS epidemic and its consequences is declared by WHO:

HIV prevention among drug addicts is an explanation of the danger of infection through injections, the provision of disposable syringes and the exchange of used ones for sterile ones. The last measures seem strange and are associated with the spread of drug addiction, but in this case it is easier to at least partially stop the ways of HIV infection than to wean great amount drug addicts.
HIV kit is useful in everyday life for everyone, at the workplace - to doctors and rescuers, as well as people in contact with HIV-infected people. Medicines are available and elementary, but their use really reduces the risk of infection with the immunodeficiency virus:
- Alcohol solution of iodine 5%;
- Ethanol 70%;
- Bandaging products (package of sterile gauze swabs, bandage, plaster) and scissors;
- Sterile distilled water - 500 ml;
- Crystals of potassium permanganate (potassium permanganate) or hydrogen peroxide 3%;
- Eye pipettes (sterile, in a package or in a case);
- Specific preparations are provided only for physicians working at blood sampling stations and in the emergency departments of hospitals.

The blood that got on the skin from an HIV-infected person, you should immediately wash it off with soap and water, then treat it with a swab dipped in alcohol. When pricked or cut through gloves they need to be removed, squeezed out blood, on the wound - hydrogen peroxide; then blot the foam, and cauterize the edges of the wound with iodine and, if necessary, apply a bandage. hit in the eyes: washing first with water, then with a solution of potassium permanganate (light pink). Oral cavity: rinse with pale pink potassium permanganate, then with 70% ethanol. After unprotected intercourse: if possible - a shower, then treatment (douching, washing) of the genital organs with a rich pink solution of potassium permanganate.
Prevention of AIDS will be more effective if each person becomes conscious of their health. It is much easier to use a condom during sexual intercourse and avoid unwanted acquaintances (prostitutes, drug addicts) than to undergo long and expensive treatment later. To understand the picture of the danger of HIV, just compare the statistics: for a year from fever ebola about 8,000 people died, and more than 1.5 million from HIV! conclusions obvious and disappointing modern world The immunodeficiency virus has become a real threat to all mankind.
Video: educational film about HIV
Video: AIDS in the program “Live healthy!”
It is a disease caused by the human immunodeficiency virus, characterized by acquired immunodeficiency syndrome, which contributes to the occurrence of secondary infections and malignant tumors due to a deep inhibition of the protective properties of the body. HIV infection has a variety of course options. The disease can last only a few months or stretch up to 20 years. The main method for diagnosing HIV infection remains the detection of specific antiviral antibodies, as well as viral RNA. Currently, patients with HIV are treated with antiretroviral drugs that can reduce the reproduction of the virus.
General information
It is a disease caused by the human immunodeficiency virus, characterized by acquired immunodeficiency syndrome, which contributes to the occurrence of secondary infections and malignant tumors due to a deep inhibition of the protective properties of the body. Today, the world is experiencing a pandemic of HIV infection, the incidence of the world's population, especially in Eastern Europe, is steadily growing.
Exciter characteristic
The human immunodeficiency virus is a DNA-containing virus that belongs to the Lentivirus genus of the Retroviridae family. There are two types: HIV-1 is the main causative agent of HIV infection, the cause of the pandemic, the development of AIDS. HIV-2 is a rare type found mainly in West Africa. HIV is an unstable virus, it dies quickly outside the carrier's body, is sensitive to temperature (reduces infectious properties at a temperature of 56 ° C, dies after 10 minutes when heated to 70-80 ° C). It is well preserved in the blood and its preparations prepared for transfusion. The antigenic structure of the virus is highly variable.
The reservoir and source of HIV infection is a person: suffering from AIDS and a carrier. Natural reservoirs of HIV-1 have not been identified, it is believed that wild chimpanzees are the natural host in nature. HIV-2 is carried by African monkeys. Susceptibility to HIV in other animal species has not been noted. The virus is found in high concentrations in blood, semen, vaginal secretions, and menstrual fluids. It can be isolated from women's milk, saliva, lacrimal secretions and cerebrospinal fluid, but these biological fluids pose a lesser epidemiological hazard.
The probability of transmission of HIV infection increases in the presence of damage to the skin and mucous membranes (injuries, abrasions, cervical erosion, stomatitis, paradontosis, etc.) HIV is transmitted using the blood contact and biocontact mechanism naturally(during sexual intercourse and vertically: from mother to child) and artificial (mainly implemented with a hemopercutaneous transmission mechanism: with transfusions, parenteral administration of substances, traumatic medical procedures).
The risk of HIV infection with a single contact with a carrier is low, regular sexual contact with an infected person significantly increases it. Vertical transmission of infection from a sick mother to a child is possible both in the prenatal period (through defects in the placental barrier) and during childbirth, when the child comes into contact with the mother's blood. In rare cases, postnatal transmission with breast milk is recorded. The incidence among children of infected mothers reaches 25-30%.
Parenteral infection occurs by injection with needles contaminated with the blood of HIV-infected persons, with blood transfusions of infected blood, non-sterile medical procedures (piercing, tattoos, medical and dental procedures performed with instruments without proper processing). HIV is not transmitted by contact-household way. Human susceptibility to HIV infection is high. The development of AIDS in people over 35 years of age usually occurs in more short time from the moment of infection. In some cases, resistance to HIV is noted, which is associated with specific immunoglobulins A present on the mucous membranes of the genital organs.
The pathogenesis of HIV infection
The human immunodeficiency virus, when it enters the blood, invades macrophages, microglia and lymphocytes, which are important in the formation of the body's immune responses. The virus destroys the ability of immune bodies to recognize their antigens as foreign, populates the cell and proceeds to reproduction. After the multiplied virus enters the bloodstream, the host cell dies, and the viruses are introduced into healthy macrophages. The syndrome develops slowly (for years), in waves.
At first, the body compensates for the mass death of immune cells by producing new ones, over time, compensation becomes insufficient, the number of lymphocytes and macrophages in the blood decreases significantly, the immune system collapses, the body becomes defenseless both against exogenous infection and bacteria inhabiting organs and tissues normal (which leads to the development of opportunistic infections). In addition, the mechanism of protection against the reproduction of defective blastocytes - malignant cells - is disrupted.
The colonization of immune cells by the virus often provokes various autoimmune conditions, in particular, neurological disorders are characteristic as a result of autoimmune damage to neurocytes, which can develop even earlier than the immunodeficiency clinic manifests itself.
Classification
In the clinical course of HIV infection, 5 stages are distinguished: incubation, primary manifestations, latent, secondary diseases and terminal. The stage of primary manifestations can be asymptomatic, in the form of primary HIV infection, and can also be combined with secondary diseases. The fourth stage, depending on the severity, is divided into periods: 4A, 4B, 4C. The periods go through phases of progression and remission, differing depending on the antiretroviral therapy taking place or its absence.
Symptoms of HIV Infection
Incubation stage (1)- can be from 3 weeks to 3 months, in rare cases it can be extended up to a year. At this time, the virus is actively multiplying, but there is no immune response to it yet. The incubation period of HIV ends either with a clinic of acute HIV infection or with the appearance of HIV antibodies in the blood. At this stage, the basis for the diagnosis of HIV infection is the detection of the virus (antigens or DNA particles) in the blood serum.
Stage of primary manifestations (2) characterized by the manifestation of the body's reaction to the active replication of the virus in the form of a clinic of acute infection and an immune response (production of specific antibodies). The second stage may be asymptomatic, the only sign of developing HIV infection will be a positive serological diagnosis for antibodies to the virus.
Clinical manifestations of the second stage proceed according to the type of acute HIV infection. The onset is acute, observed in 50-90% of patients three months after the moment of infection, often preceding the formation of HIV antibodies. Acute infection without secondary pathologies has a rather diverse course: fever, a variety of polymorphic rashes on the skin and visible mucous membranes, polylymphadenitis, pharyngitis, lienal syndrome, and diarrhea may occur.
In 10-15% of patients, acute HIV infection occurs with the addition of secondary diseases, which is associated with a decrease in immunity. These can be tonsillitis, pneumonia of various origins, fungal infections, herpes, etc.
Acute HIV infection usually lasts from several days to several months, averaging 2-3 weeks, after which, in the vast majority of cases, it passes into a latent stage.
Latent stage (3) characterized by a gradual increase in immunodeficiency. The death of immune cells at this stage is compensated by their increased production. At this time, HIV can be diagnosed using serological tests (antibodies to HIV are present in the blood). The clinical sign may be enlargement of several lymph nodes from different, unrelated groups, excluding inguinal lymph nodes. At the same time, others pathological changes enlarged lymph nodes (soreness, changes in surrounding tissues) are not observed. The latent stage can last from 2-3 years, up to 20 or more. On average, it lasts 6-7 years.
Stage of secondary diseases (4) characterized by the occurrence of concomitant (opportunistic) infections of viral, bacterial, fungal, protozoal genesis, malignant tumors against the background of severe immunodeficiency. Depending on the severity of secondary diseases, 3 periods of the course are distinguished.
- 4A - weight loss does not exceed 10%, infectious (bacterial, viral and fungal) lesions of integumentary tissues (skin and mucous membranes) are noted. The performance is reduced.
- 4B - weight loss of more than 10% of the total body weight, prolonged temperature reaction, prolonged diarrhea that does not have an organic cause is possible, pulmonary tuberculosis may join, infectious diseases recur and progress, localized Kaposi's sarcoma, hairy leukoplakia is detected.
- 4B - general cachexia is noted, secondary infections acquire generalized forms, candidiasis of the esophagus, respiratory tract, pneumocystis pneumonia, tuberculosis of extrapulmonary forms, disseminated Kaposi's sarcoma, neurological disorders are noted.
Substages of secondary diseases go through phases of progression and remission, which differ depending on the presence of antiretroviral therapy or its absence. In the terminal stage of HIV infection, secondary diseases that have developed in a patient become irreversible, treatment measures lose their effectiveness, and death occurs after a few months.
The course of HIV infection is quite diverse, not always all stages take place, certain clinical signs may be absent. Depending on the individual clinical course, the duration of the disease can range from several months to 15-20 years.
Clinical features of HIV infection in children
HIV in early childhood contributes to delayed physical and psychomotor development. Recurrence of bacterial infections in children is noted more often than in adults, lymphoid pneumonitis, an increase in pulmonary lymph nodes, various encephalopathies, and anemia are not uncommon. common cause infant mortality in HIV infections is hemorrhagic syndrome, which is a consequence of severe thrombocytopenia.
The most common clinical manifestation of HIV infection in children is a delay in the pace of psychomotor and physical development. HIV infection received by children from mothers ante- and perinatally proceeds much more severely and progresses faster, in contrast to that in children infected after a year.
Diagnostics
Currently, the main diagnostic method for HIV infection is the detection of antibodies to the virus, which is carried out mainly using the ELISA technique. In the case of a positive result, the blood serum is examined using the immune blotting technique. This makes it possible to identify antibodies to specific HIV antigens, which is a sufficient criterion for the final diagnosis. Failure to blot detect antibodies of a characteristic molecular weight, however, does not rule out HIV. During the incubation period, the immune response to the introduction of the virus has not yet been formed, and in the terminal stage, as a result of severe immunodeficiency, antibodies cease to be produced.
When HIV is suspected and no positive immune blotting results are available, PCR is an effective method for detecting viral RNA particles. HIV infection diagnosed by serological and virological methods is an indication for dynamic monitoring of the state of the immune status.
Treatment of HIV infection
Therapy of HIV-infected persons implies constant monitoring of the body's immune status, prevention and treatment of emerging secondary infections, and control over the development of neoplasms. Often, HIV-infected persons require psychological assistance and social adaptation. Currently, due to the significant spread and high social significance of the disease on a national and global scale, support and rehabilitation of patients is being carried out, access to social programs is expanding that provides patients with medical care that facilitates the course and improves the quality of life of patients.
To date, the predominant etiotropic treatment is the appointment of drugs that reduce the reproductive ability of the virus. Antiretroviral drugs include:
- NRTIs (nucleoside transcriptase inhibitors) of various groups: zidovudine, stavudine, zalcitabine, didanosine, abacavir, combination drugs;
- NTRTs (nucleotide reverse transcriptase inhibitors): nevirapine, efavirenz;
- protease inhibitors: ritonavir, saquinavir, darunavir, nelfinavir and others;
- fusion inhibitors.
When deciding to start antiviral therapy, patients should remember that the use of drugs is carried out for many years, almost for life. The success of therapy directly depends on strict adherence to the recommendations: timely regular intake of drugs in the required dosages, adherence to the prescribed diet and strict adherence to the regimen.
Occurring opportunistic infections are treated in accordance with the rules of effective therapy against the pathogen that caused them (antibacterial, antifungal, antiviral agents). Immunostimulating therapy for HIV infection is not used, since it contributes to its progression, cytostatics prescribed for malignant tumors depress the immune system.
Treatment of HIV-infected people includes general strengthening and supporting the body means (vitamins and biologically active substances) and methods of physiotherapeutic prevention of secondary diseases. Patients suffering from drug addiction are recommended to be treated in appropriate dispensaries. Due to significant psychological discomfort, many patients undergo long-term psychological adaptation.
Forecast
HIV infection is completely incurable, in many cases antiviral therapy gives little result. Today, on average, HIV-infected people live 11-12 years, but careful therapy and modern medications will significantly lengthen the life of patients. The main role in curbing the developing AIDS is played by the psychological state of the patient and his efforts to comply with the prescribed regimen.
Prevention
Currently, the World Health Organization is conducting general preventive measures to reduce the incidence of HIV infection in four main areas:
- education on the safety of sexual relations, distribution of condoms, treatment of sexually transmitted diseases, promotion of a culture of sexual relations;
- control over the manufacture of drugs from donor blood;
- managing the pregnancy of HIV-infected women, providing them with medical care and providing them with chemoprophylaxis (in the last trimester of pregnancy and during childbirth, women receive antiretroviral drugs, which are also prescribed for newborn children for the first three months of life);
- organization of psychological and social assistance and support for HIV-infected citizens, counseling.
Currently, in world practice, special attention is paid to such epidemiologically important factors in relation to the incidence of HIV infection as drug addiction, disorderly sex life. As a preventive measure, many countries provide free distribution of disposable syringes and methadone substitution therapy. As a measure to reduce sexual illiteracy, courses on sexual hygiene are being introduced into curricula.
Chapter 19. HIV INFECTION
Chapter 19. HIV INFECTION
HIV infection is a chronic progressive human disease caused by a retrovirus, in which the immune system is affected and an immunodeficiency state is formed, leading to the development of opportunistic and secondary infections, as well as malignant tumors.
19.1. ETIOLOGY
Pathogen this disease isolated in 1983 and named human immunodeficiency virus - HIV (Human Immunodeficiency Virus - HIV). The virus belongs to the retrovirus family.
Currently, 2 strains of the human immunodeficiency virus are known: HIV-1 and HIV-2.
The virus particle has a size of about 100 nm and is a core surrounded by a shell. The nucleus contains RNA and a special enzyme (reverse transcriptase, or reversetase), due to which the genetic material of the virus is integrated into the DNA of the host cell, which leads to further reproduction of the virus and cell death. The shell of the viral particle contains the glycoprotein gp120, which determines the tropism of the virus to the cells of the human body that have CD4 + receptors.
Like all retroviruses, HIV is unstable in the external environment, is completely inactivated by heating at 56 °C for 30 minutes, dies when boiled or when the reaction of the environment changes (pH below 0.1 and above 13), as well as when exposed to traditional disinfectants ( solutions of 3-5% chloramine, 3% bleach, 5% lysol, 70% ethyl alcohol, etc.). In biological fluids (blood, semen), the virus can be stored for a long time in a dried or frozen state.
19.2. EPIDEMIOLOGY
The incubation period lasts about 1 month.
The source of infection is an HIV-infected person, both at the stage of asymptomatic carriage and with advanced clinical manifestations of the disease.
AT most The virus has been found in blood, semen, cerebrospinal fluid, breast milk, vaginal and cervical secretions, and biopsies of various tissues. In a small amount, insufficient for infection, it is found in saliva, lacrimal fluid, and urine.
Ways of transmission of HIV: contact-sexual and parenteral.
The contact-sexual route of transmission is characterized by the penetration of the virus into the body through damaged skin and mucous membranes (which are abundantly supplied with blood and have a high absorption capacity). The unaffected epidermis is practically impermeable to viral particles.
The sexual route of transmission is observed during sexual intercourse (hetero- and homosexual) and is apparently associated with microtrauma of the mucous membranes, which is especially great with anogenital and orogenital contacts, as well as in the presence of inflammatory diseases of the genital organs.
The parenteral route of transmission is characterized by the entry of the virus directly into the bloodstream and occurs during blood transfusions of infected blood or its components, injections using contaminated instruments, especially when using drugs, transplants of donor organs and tissues.
Child infection most often occurs transplacental during pregnancy or during childbirth. It was noted that in children born to HIV-infected mothers, the disease develops only in 25-40% of cases, which is associated with the mother's condition and obstetric interventions. Thus, a high concentration of the virus in the blood or AIDS in the mother, prematurity of the child, natural childbirth and exposure of the child to maternal blood increase the risk of HIV transmission, but none of these factors predicts the likelihood of a child becoming infected. Infection of a child can also occur when feeding HIV-infected mother chest, as well as expressed breast milk.
At-risk groups(most frequently infected): drug addicts, homosexuals and bisexuals, prostitutes, as well as those prone to frequent change of sexual partners.
19.3. PATHOGENESIS
Having penetrated into the body, the virus, using the gp120 glycoprotein, is fixed on the membrane of cells with CD4 + receptors. These receptors are located mainly on T-helper lymphocytes, which play a major role in the development of the immune response, as well as on monocytes, macrophages, and some other cells. From the surface of cells, it penetrates deep into the RNA of the virus, is transformed with the help of the reverse transcriptase enzyme into the DNA of the cell, and new viral particles are synthesized, leading to the death of T-lymphocytes. Infected monocytes, unlike lymphocytes, do not die, but serve reservoir latent infection.
With HIV infection in the body, the ratio of T-helpers and T-suppressors is disturbed. The defeat of T-helpers entails a decrease in the activity of macrophages and natural killers, the production of antibodies by B-lymphocytes decreases, which results in a pronounced weakening of the immune response.
The result of an immunodeficiency state is the development of various opportunistic infections, secondary infection, and malignant neoplasms.
19.4. CLASSIFICATION OF HIV INFECTION
According to the classification of V.I. Pokrovsky, since 1989, 5 stages of HIV infection have been distinguished.
Incubation period
The incubation period is 2-8 weeks. There are no clinical manifestations, but an HIV-infected person can be a source of infection. Antibodies to the virus have not yet been determined.
Primary manifest (acute) period
In 50% of patients, the disease begins with non-specific clinical manifestations: fever, myalgia and arthralgia, lymphadenopathy, nausea, vomiting, diarrhea, skin rashes, etc.
In some patients, this period of the disease is asymptomatic.
The virus in the blood is determined by PCR. Antibodies to HIV may not yet be detected.
latent period
The latent period lasts several years (from 1 year to 8-10 years). There are no clinical manifestations, the immune status does not change, but the person is the source of infection (there is a virus carrier). Detect antibodies to HIV using the method ELISA and reactions immunoblotting.
At the end of the latent period, generalized lymphadenopathy develops. Diagnostic value is an increase (more than 1 cm) of two or more lymph nodes (except inguinal) in unrelated areas for more than 3 months.
AIDS (stage of secondary diseases)
The main clinical manifestations of AIDS are fever, night sweats, fatigue, weight loss (up to cachexia), diarrhea, generalized lymphadenopathy, hepatosplenomegaly, pneumocystis pneumonia, progressive neurological disorders, candidiasis of internal organs, lymphomas, Kaposi's sarcoma, opportunistic and secondary infections.
terminal stage
Increasing cachexia, general intoxication, dementia, progressing intercurrent diseases. The process ends in death.
19.5. SKIN MANIFESTATIONS IN AIDS
Distinctive features of skin diseases in AIDS are a long relapsing course, the widespread nature of rashes, atypical localization, an unusual age period, and the poor effectiveness of conventional therapy.
Mycoses
The development of fungal diseases in HIV-infected patients is an early clinical symptom of an immunodeficiency state.
Candidiasis of the skin and mucous membranes
Candidiasis of the skin and mucous membranes occurs in almost all patients with AIDS. Most often manifested by candidiasis of the mucous membranes of the oral cavity, cheilitis, esophagitis, candidiasis of large folds (yeast diaper rash), damage to the anogenital region, candidiasis of the external auditory canal, damage to the nail folds (candidiasis paronychia), nail plates.
Features of the course of candidiasis in AIDS - the defeat of young people, especially men, a tendency to form extensive lesions, a tendency to erosion and ulceration.
Rubrophytia
Rubrophytosis is a common form of mycosis of smooth skin in AIDS patients. During the course of the disease, attention is drawn to the prevalence of rashes, the appearance of infiltrated elements, and on microscopic examination, the abundance of mycelium.
Seborrheic dermatitis and versicolor
Seborrheic dermatitis and versicolor - diseases belonging to the group of malacezioses and caused by yeast-like lipophilic flora Malassezia furfur.
Seborrheic dermatitis
Seborrheic dermatitis is detected in more than half of HIV-infected people already in the early period. Usually the disease begins with seborrheic zones (face, scalp, auricles, etc.), and then spreads to the skin of the trunk, upper and lower extremities (up to erythroderma). Rashes are accompanied by abundant peeling, the formation of crusts, erosion occurs in the folds, and hair falls out.
versicolor
Pityriasis versicolor in HIV-infected people is characterized by the appearance on the skin of large infiltrated spots that transform into plaques.
Viral skin diseases
Herpes simplex
Herpes simplex is a typical disease in HIV-infected patients and occurs with frequent relapses, almost without remissions. It is distinguished by an abundance of elements, up to a disseminated lesion, as well as a tendency to erosion and ulceration, accompanied by severe pain. Often, scars form at the sites of rashes. With repeated use of acyclovir, the resistance of the virus to this drug quickly develops.
Shingles
Herpes zoster on the background of HIV infection acquires a relapsing course, which is extremely rare in young patients and is an early marker of an immunosuppressive state. The recurrent form of herpes zoster in persons under 60 years of age is currently considered as one of the HIV-indicative diseases (especially if patients have persistent lymphadenopathy).
Clinically, the disease is characterized by prevalence, frequent development of gangrenous (necrotic) forms, severe pain, prolonged neuralgia, and scarring.
molluscum contagiosum
molluscum contagiosum - a viral disease, more characteristic of younger children, is very common among HIV-infected patients, in whom it acquires a disseminated relapsing character. The most frequent localization of rashes is the face, neck, scalp, where the elements become large (more than 1 cm), confluent.
Hairy leukoplakia of the oral cavity
Hairy leukoplakia of the oral cavity - the disease, described only in HIV-infected patients, is caused by the Epstein-Barr virus and papillomavirus. Clinically it is a thickening
mucous membrane of the lateral surface of the tongue in the form of a whitish plaque covered with thin keratotic hairs, the length of which is several millimeters.
warts
Warts are caused by different types of human papillomavirus. In HIV-infected patients, more often than in the general population, common forms of vulgaris, palmar-plantar and anogenital ( genital warts) warts.
pyoderma
Pyoderma is common in AIDS patients. They are characterized by a severe course and often lead to the development of sepsis. The most typical development of folliculitis, furunculosis, ecthyma, rupioid pyoderma, chronic diffuse streptoderma, ulcerative vegetative pyoderma and other forms. In some cases, atypical pyoderma caused by gram-negative flora is observed.
Scabies
Scabies against the background of an immunodeficiency state proceeds very hard - in the form of Norwegian scabies, which is characterized by high contagiousness for others, and clinically by widespread localization of rashes, massive cortical layers, and a violation of the general condition.
skin tumors
Kaposi's sarcoma, a malignant tumor of the blood vessels, is a significant clinical manifestation of HIV infection. The disease is considered as an AIDS-defining disease. It is characterized by the appearance on the skin, mucous membranes, internal organs of vascular nodules of a dark cherry or black color. Unlike the classic type of Kaposi's sarcoma (which occurs in elderly patients, is characterized by a slow development of the clinical picture, rare involvement of internal organs in the process and a typical initial localization on the feet and legs), AIDS-associated Kaposi's sarcoma, on the contrary, affects young and middle-aged people. age, characterized by a malignant course with meta-
tumor stasis in internal organs (lungs, bones, brain, etc.), and primary rashes can appear not only on the shins, but also on the face, scalp, auricles, oral mucosa (Fig. 19-1, 19-2).
Drug toxicoderma
Drug toxicoderma in HIV-infected people usually develops during therapy with co-trimoxazole and proceeds in a measles-like type. This reaction develops in 70% of patients.
Rice. 19-1. Kaposi's sarcoma on the foot

Rice. 19-2. Kaposi's sarcoma on the leg
19.6. FEATURES OF THE COURSE OF HIV INFECTION IN CHILDREN
Infection of children occurs mainly by vertical transmission (from an HIV-infected mother to her child): in utero, during childbirth or during breastfeeding.
Children born to HIV-infected mothers fall ill in 25-40% of cases. When children are born from seropositive mothers, it can be difficult to decide whether the child has HIV infection, since newborns are usually seropositive (maternal antibodies in the child's blood last up to 18 months), regardless of whether they are infected or not. In children younger than one and a half years of age, the diagnosis of HIV is confirmed by the detection of viral nucleic acids by PCR.
The first clinical manifestations of HIV infection in a child with perinatal infection occur no earlier than 4 months of age. In most children, the asymptomatic period lasts longer - on average, about 5 years.
The most typical skin lesions in children are candidiasis of the mucous membrane of the oral cavity and esophagus, seborrheic dermatitis, as well as staphyloderma, herpetic gingivostomatitis, common giant molluscum contagiosum, onychomycosis. Children often develop a hemorrhagic rash (petechial or purpuric) that develops against a background of thrombocytopenia.
Kaposi's sarcoma and other malignant neoplasms are not typical for childhood.
19.7. LABORATORY RESEARCH
Methods for detecting the presence of antibodies to HIV
The selection method is the enzyme-linked immunosorbent assay (ELISA), in which 3 months after infection, antibodies to HIV are determined in 90-95% of patients. In the terminal stage, the number of antibodies may decrease until complete disappearance.
To confirm the ELISA data, a method is used immunoblotting, in which antibodies are detected certain proteins of the virus. This method rarely gives false positive results.
Methods that determine the presence of viral particles in the blood
The PCR method allows you to determine the number of copies of HIV RNA in 1 µl of blood plasma. The presence of any number of viral particles in the serum
blood flow proves HIV infection. This method is also used to determine the effectiveness of antiviral treatment.
Methods to assess the state of immunity
Determine the number of T-helpers (CD4) and T-suppressors (CD8), as well as their ratio. Normally, T-helpers are more than 500 cells per µl, and the CD4/CD8 ratio is 1.8-2.1. With HIV infection, the number of T-helpers is significantly reduced and the ratio is less than 1.
19.8. DIAGNOSTICS
Diagnosis is based on characteristic complaints (loss of body weight, increased fatigue, cough, diarrhea, prolonged fever, etc.), clinical picture (detection of drug addiction stigmas, lymphadenopathy, the presence of AIDS-associated dermatoses and other infectious and opportunistic infections), as well as laboratory research data.
19.9. TREATMENT
Three classes of antiretroviral drugs are used to treat HIV infection.
Nucleoside reverse transcriptase inhibitors (zidovudine 200 mg orally 4 times a day, for children the dose is calculated based on 90-180 mg/m 2 orally 3-4 times a day; didanosine 200 mg orally
2 times a day, for children - 120 mg / m 2 orally 2 times a day; as well as stravudine, lamivudine, etc.
Non-nucleoside reverse transcriptase inhibitors (zalcitabine 0.75 mg orally 3 times a day, for children - 0.01 mg/kg orally
3 times a day; abacavir 300 mg orally 2 times a day, for children - 8 mg/kg orally 2 times a day.
HIV protease inhibitors (nelfinavir 750 mg orally 3 times a day, for children - 20-30 mg / kg 3 times a day; ritonavir 600 mg 2 times a day, for children - 400 mg / m 2 orally 2 times per day, as well as saquinavir, amprenavir, etc.
The most effective regimens that include 2 nucleoside reverse transcriptase inhibitors in combination with an inhibitor
protease or with a non-nucleoside reverse transcriptase inhibitor.
HIV-infected patients are treated for malignant tumors and opportunistic infections.
19.10. CONSULTING
Preventive measures include the promotion of safe sex, the fight against drug addiction, the observance of the sanitary and anti-epidemic regime in medical institutions, the examination of donors, etc.
To prevent infection of children, a planned examination of pregnant women for HIV infection is necessary. If a disease is detected in a pregnant woman, antiviral treatment should be prescribed to her, which reduces the risk of morbidity in a child to 8%. Delivery to HIV-infected women is carried out by caesarean section. From breastfeeding the child must be abandoned.
Dermatovenereology: a textbook for students of higher educational institutions / V. V. Chebotarev, O. B. Tamrazova, N. V. Chebotareva, A. V. Odinets. -2013. - 584 p. : ill.